De Quervain Tenosynovitis: Anatomical Variants of the First Dorsal Compartment and Their Role in Ultrasound-Guided Injection and Surgical Management — A Narrative Review
DOI:
https://doi.org/10.56929/jseaortho-2026-0309Keywords:
De Quervain tenosynovitis, first dorsal compartment, anatomical variant, ultrasonography, abductor pollicis longus, extensor pollicis brevisAbstract
Purpose: De Quervain tenosynovitis is a common cause of radial wrist pain and is characterized by stenosing tendinopathy of the abductor pollicis longus and extensor pollicis brevis in the first dorsal compartment. Increasing evidence suggests that the anatomical variants within this compartment contribute to disease development and treatment failure. To summarize the current evidence on anatomical variations in the first dorsal wrist compartment, their detection using ultrasound, and their implications for injection-based and surgical management of de Quervain tenosynovitis.
Methods: Studies published between 2015 and 2025 on de Quervain stenosynovitis, first dorsal compartment anatomy, ultrasonography, injection therapy, and surgical outcomes were included.
Results: Inter-tendinous septation and subcompartmentalization of the abductor pollicis longus and extensor pollicis brevis tendons were more prevalent in patients with de Quervain tenosynovitis than in controls and were associated with persistent symptoms after conventional corticosteroid injection or surgical release. Ultrasound demonstrates high sensitivity and specificity for detecting septa, multiple tendon slips, and subcompartments and reliably maps adjacent neurovascular structures. Ultrasound-guided corticosteroid injections, hydrodissection, platelet-rich plasma injection, and percutaneous release techniques have shown improved targeting of pathological compartments and favorable clinical outcomes. In surgical management, failure to recognize and decompress the separate subcompartments is a key cause of residual pain and recurrence.
Conclusions: Anatomical variants of the first dorsal compartment are common and clinically significant in de Quervain stenosynovitis. The routine use of ultrasound to identify anatomical variants can optimize the selection and execution of both nonsurgical and surgical treatments, potentially improving outcomes and reducing recurrence.
Metrics
References
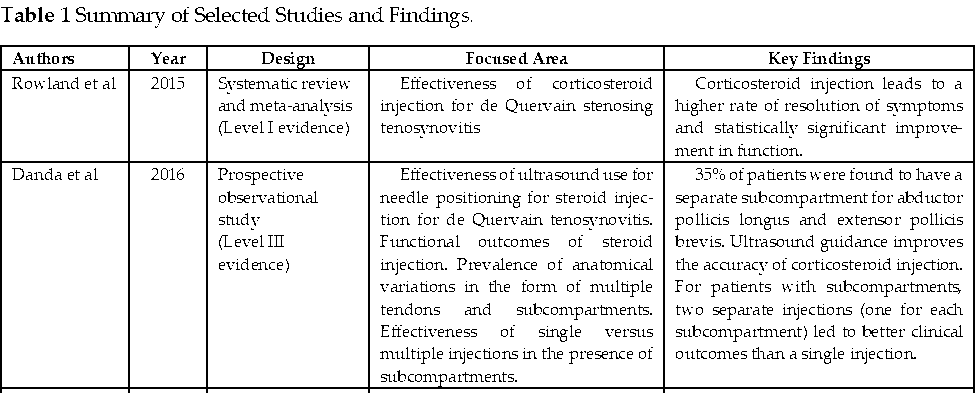
Rowland P, Phelan N, Gardiner S, et al. The effectiveness of corticosteroid injection for De Quervain's stenosing tenosynovitis (DQST): A systematic review and meta-analysis. Open Orthop J 2015;9:437-44. DOI: https://doi.org/10.2174/1874325001509010437
Challoumas D, Ramasubbu R, Rooney E, et al. Management of de Quervain's tenosynovitis: A systematic review and network meta-analysis. JAMA Netw Open 2023;6:e2337001. DOI: https://doi.org/10.1001/jamanetworkopen.2023.37001
Fakoya AO, Tarzian M, Sabater EL, et al. De Quervain’s disease: A discourse on etiology, diagnosis, and treatment. cureus 2023;15:e38079. DOI: https://doi.org/10.7759/cureus.38079
Irfan S, Butt M, Ahmed I, et al. Prevalence of dequervain's tenosynovitis among clinical physical therapists in islamabad: A cross-sectional study. Pak J Med Health Sci 2023;17:42-5. DOI: https://doi.org/10.53350/pjmhs202317542
Abi-Rafeh J, Mojtahed Jaberi M, Kazan R, et al. Utility of ultrasonography and significance of surgical anatomy in the management of de Quervain disease: A systematic review and meta-analysis. Plast Reconstr Surg 2022;149:420-34. DOI: https://doi.org/10.1097/PRS.0000000000008792
Allbrook V. ‘The side of my wrist hurts’: De Quervain’s tenosynovitis. Aust J Gen Pract. 2019;48:753-6. DOI: https://doi.org/10.31128/AJGP-07-19-5018
Hsu CY, Ke DS, Lin CL, et al. Association between de Quervain syndrome and herpes zoster: A population-based cohort study. BMJ Open 2021;11:e046891. DOI: https://doi.org/10.1136/bmjopen-2020-046891
Sharif MS, Alam MM, Akhtar MW, et al. Prevalence of dequervains tenosynovitis in 20-40 years old mobile users. J Health Rehabil Res 2024;4:1153-7. DOI: https://doi.org/10.61919/jhrr.v4i1.561
Ramchandani J, Thakker A, Tharmaraja T. Time to reconsider occupation induced de Quervain’s tenosynovitis: An updated review of risk factors. Orthop Rev (Pavia) 2022;14:36911. DOI: https://doi.org/10.52965/001c.36911
Garçon JJ, Charruau B, Marteau E, et al. Results of surgical treatment of De Quervain’s tenosynovitis: 80 cases with a mean follow-up of 9.5 years. Orthop Traumatol Surg Res 2018;104:893-6. DOI: https://doi.org/10.1016/j.otsr.2018.04.022
Le Viet D, Lantieri L. [De Quervain’s tenosynovitis. Transversal scar and fixation of the capsular flap]. Rev Chir Orthop Reparatrice Appar Mot 1992;78:101-6.
Liu C, Moye S, Blazar P, et al. Anatomical variations of the first dorsal compartment in de Quervain tenosynovitis. Hand (N Y) 2024;19:1159-65. DOI: https://doi.org/10.1177/15589447231164746
Marth T, Grob NA, Jacobson JA, et al. Tendon anatomy and tendon disorders of the wrist. Rofo 2025;197:1148-61. DOI: https://doi.org/10.1055/a-2499-5875
Kotzias D, Koutserimpas C, Chrysikos D, et al. Clinical considerations of first extensor wrist compartment (FEWC) variants and de Quervain’s disease: A review study. Cureus 2023;15:e42124. DOI: https://doi.org/10.7759/cureus.42124
Jackson WT, Viegas SF, Coon TM, et al. Anatomical variations in the first extensor compartment of the wrist. A clinical and anatomical study. J Bone Joint Surg Am 1986;68:923-6. DOI: https://doi.org/10.2106/00004623-198668060-00016
Gonzalez MH, Sohlberg R, Brown A, et al. The first dorsal extensor compartment: An anatomic study. J Hand Surg Am 1995;20:657-60. DOI: https://doi.org/10.1016/S0363-5023(05)80286-2
Bahm J, Szabo Z, Foucher G. The anatomy of de Quervain's disease. A study of operative findings. Int Orthop 1995;19:209-11. DOI: https://doi.org/10.1007/BF00185223
Lee ZH, Stranix JT, Anzai L, Sharma S. Surgical anatomy of the first extensor compartment: A systematic review and comparison of normal cadavers vs. De Quervain syndrome patients. J Plast Reconstr Aesthet Surg 2017;70:127-31. DOI: https://doi.org/10.1016/j.bjps.2016.08.020
Lee HJ, Kim PT, Aminata IW, et al. Surgical release of the first extensor compartment for refractory de Quervain's tenosynovitis: surgical findings and functional evaluation using DASH scores. Clin Orthop Surg 2014;6:405-9. DOI: https://doi.org/10.4055/cios.2014.6.4.405
Ahmad I, Hussain K, Khan Z, et al. Intra operative Anatomical variations of the first extensor compartment of the wrist in patients of de Quervain’s disease. J Pak Orthop Assoc 2020;32:153-7.
Croutzet P, Guinand R, Mares O, et al. Ultrasound-guided de Quervain’s tendon release, feasibility, and first outcomes. J Wrist Surg 2019;8:513-9. DOI: https://doi.org/10.1055/s-0039-1678688
Danda RS, Kamath J, Jayasheelan N, et al. Role of guided ultrasound in the treatment of de Quervain tenosynovitis by local steroid infiltration. J Hand Microsurg 2016;8:34-7. DOI: https://doi.org/10.1055/s-0036-1581123
Lee YS, Choi WS, Baek SH, et al. Comparative analysis of ultrasound and surgical findings in anatomical variations of de Quervain’s disease. Clin Orthop Surg 2025;17:308-16. DOI: https://doi.org/10.4055/cios24127
Ilyas AM. Nonsurgical treatment for de Quervain’s tenosynovitis. J Hand Surg 2009;34:928-9. DOI: https://doi.org/10.1016/j.jhsa.2008.12.030
Vita F, Origlio F, Pederiva D, et al. Efficacy of ultrasound-guided hydrodissection for treating De Quervain’s tenosynovitis. JPRAS Open 2024;41:148-58. DOI: https://doi.org/10.1016/j.jpra.2024.06.002
McDermott JD, Ilyas AM, Nazarian LN, et al. Ultrasound-guided injections for de Quervain’s tenosynovitis. Clin Orthop Relat Res 2012;470:1925-31. DOI: https://doi.org/10.1007/s11999-012-2369-5
Jung HS, Baek SH, Lee JS. Is a steroid injection in both compartments more effective than an injection in the extensor pollicis brevis subcompartment alone in patients with de Quervain disease? A randomized, controlled trial. Clin Orthop Relat Res 2022;480:762-70. DOI: https://doi.org/10.1097/CORR.0000000000002018
Asaad SK, Mahmood KA, Arif SO, et al. Efficacy of ultrasound‑guided platelet rich plasma injection for the management of de Quervain’s tenosynovitis. Med Int (Lond) 2023;3:12. DOI: https://doi.org/10.3892/mi.2023.72
Shen Y, Zhou Q, Sun X, et al. Percutaneous Release of the first extensor tendon compartment in de Quervain’s disease by acupotomy with US-guidance: A cadaveric study. J Pain Res 2022; 15:3995-4005. DOI: https://doi.org/10.2147/JPR.S375309
Güleç A, Türkmen F, Toker S, et al. Percutaneous release of the first dorsal extensor compartment: A cadaver study. Plast Reconstr Surg Glob Open 2016;4:e1022. DOI: https://doi.org/10.1097/GOX.0000000000001022
Bosman R, Duraku LS, Van Der Oest MJW, et al. Surgical treatment outcome of de Quervain’s disease: A systematic review and meta-analysis. Plast Reconstr Surg Glob Open 2022;10:e4305. DOI: https://doi.org/10.1097/GOX.0000000000004305
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 The Royal College of Orthopaedic Surgeons of Thailand

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.