Risk Factors for Postoperative Sciatic Nerve Injury Following Open Reduction and Internal Fixation of Acetabular Fractures: A Systematic Review and Meta-Analysis
DOI:
https://doi.org/10.56929/jseaortho-2026-0308Keywords:
acetabular fracture, sciatic nerve injury, open reduction internal fixation, risk factors, systematic review, meta-analysisAbstract
Purpose: Postoperative sciatic nerve injury is a debilitating complication after open reduction and internal fixation (ORIF) of acetabular fractures. The reported incidence and risk factors are highly variable. This systematic review and meta-analysis aimed to synthesize the current evidence on the incidence and risk factors of this complication.
Methods: A systematic search was conducted in the PubMed/MEDLINE and Scopus databases for studies published January 2000–December 2025. We included cohort and case-control studies that reported new-onset postoperative sciatic nerve injuries after acetabular ORIF. Studies not distinguishing between pre-(traumatic) and postoperative injuries were excluded. A random-effects meta-analysis using the Restricted Maximum-Likelihood estimator and Hartung-Knapp-Sidik-Jonkman adjustment was performed to pool incidence. Risk factors were analyzed by pooling unadjusted odds ratios (ORs) and narratively synthesizing adjusted ORs.
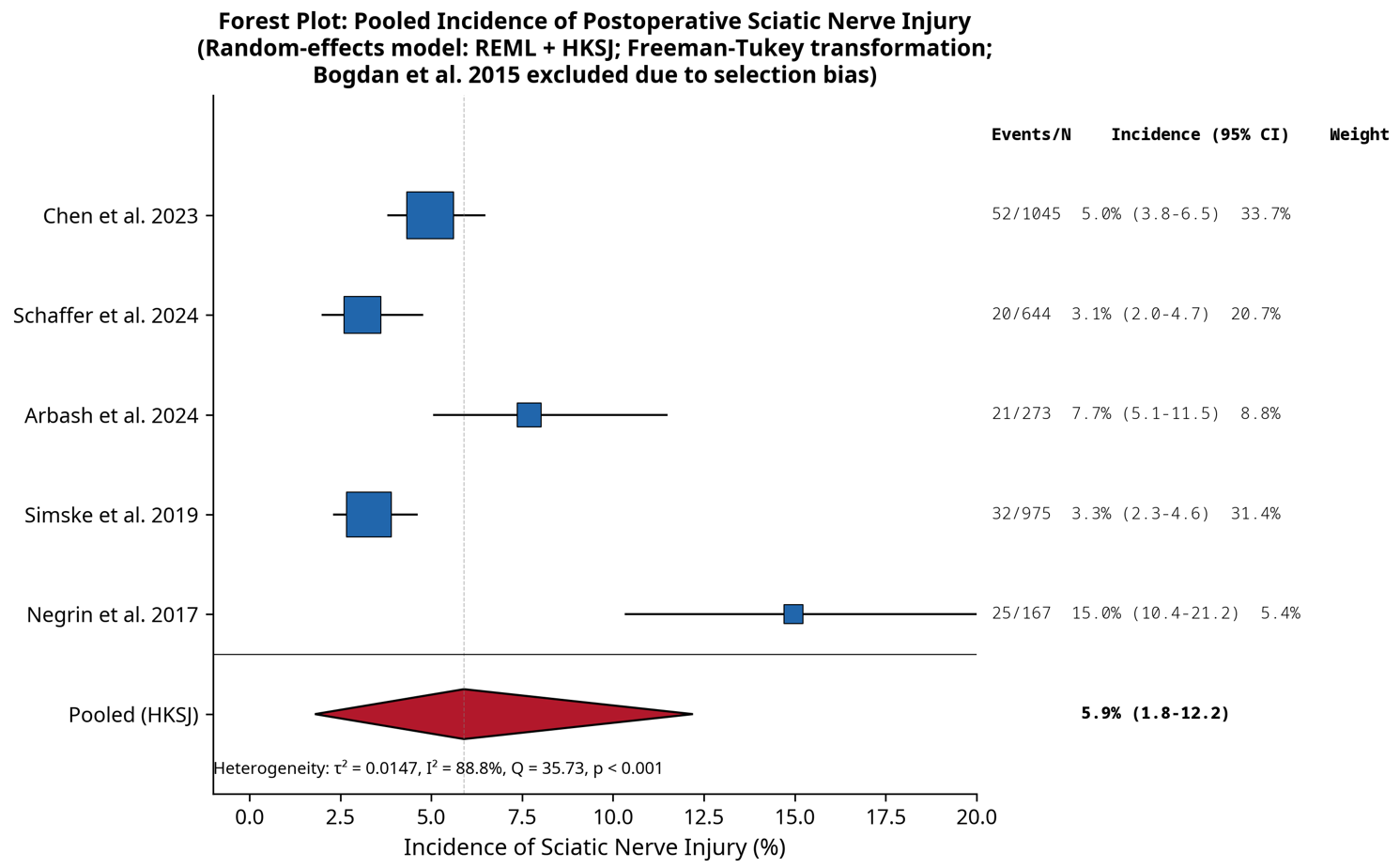
Results: Five retrospective cohort studies involving 3,104 patients were included. The pooled incidence of postoperative sciatic nerve injury was 5.9% (95% confidence interval [CI]: 1.8%–12.2%) with substantial heterogeneity (I²=88.8%). Analysis of potential risk factors, including patient positioning (prone vs. lateral), was inconclusive because of the limited number of studies and extreme statistical uncertainty. These findings should be considered exploratory and hypothesis-generating rather than definitive. Several risk factors were identified from single studies, including transverse fracture patterns (unadjusted OR 3.00, 95%CI: 1.10–7.90) and obesity (unadjusted OR 3.35, 95%CI: 1.61–6.96), but these require further validation. Leave-one-out sensitivity analysis identified one study as a major source of heterogeneity.
Conclusions: The incidence of sciatic nerve injury after acetabular ORIF was approximately 6%; however, this was based on highly heterogeneous retrospective evidence. The current literature is insufficient to support definitive conclusions regarding specific risk factors. There is an urgent need for high-quality, prospective, multicenter studies with standardized definitions to better delineate risks and guide preventative strategies.
Level of evidence: Level III (Oxford Centre for Evidence-Based Medicine 2011).
Metrics
References
Arbash MA, Algarni AD, Abalkhail MJ, et al. Sciatic nerve injury following operative fixation of acetabular fractures: a retrospective analysis. Injury 2024;55:111345.
Birkmeyer JD, Stukel TA, Siewers AE, et al. Surgeon volume and operative mortality in the United States. N Engl J Med 2003;349:2117-27. DOI: https://doi.org/10.1056/NEJMsa035205
Bogdan Y, Tornetta P III, Engel EC, et al. Neurologic injury after operative acetabular fracture fixation. J Orthop Trauma 2015;29:475-80. DOI: https://doi.org/10.1097/BOT.0000000000000362
Chen AT, Vallier HA. Sciatic and femoral nerve injuries after operative management of acetabular fractures. J Bone Joint Surg Am 2023;105:193-201.
Freeman MF, Tukey JW. Transformations related to the angular and the square root. Ann Math Statist 1950;21:607-11. DOI: https://doi.org/10.1214/aoms/1177729756
Giannoudis PV, Grotz MR, Papakostidis C, et al. Operative treatment of displaced fractures of the acetabulum: a meta-analysis. J Bone Joint Surg Br 2005;87:2-9. DOI: https://doi.org/10.1302/0301-620X.87B1.15605
Hartung J, Knapp G. A refined method for the meta-analysis of controlled clinical trials with binary outcome. Stat Med 2001;20:3875-89. DOI: https://doi.org/10.1002/sim.1009
Helfet DL, Schmeling GJ. Management of complex acetabular fractures through single nonextensile exposures. Clin Orthop Relat Res 1994;(305):58-68. DOI: https://doi.org/10.1097/00003086-199408000-00009
Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. BMJ 2003;327:557-60. DOI: https://doi.org/10.1136/bmj.327.7414.557
Judet R, Judet J, Letournel E. Fractures of the acetabulum: classification and surgical approaches for open reduction. J Bone Joint Surg Am 1964;46:1615-46. DOI: https://doi.org/10.2106/00004623-196446080-00001
Letournel E, Judet R. Fractures of the Acetabulum. 2nd ed. Berlin: Springer-Verlag; 1993. DOI: https://doi.org/10.1007/978-3-642-75435-7
Matta JM. Fractures of the acetabulum: accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg Am 1996;78:1632-45. DOI: https://doi.org/10.2106/00004623-199611000-00002
Mears DC. Surgical treatment of acetabular fractures in elderly patients with osteoporotic bone. J Am Acad Orthop Surg 1999;7:128-41. DOI: https://doi.org/10.5435/00124635-199903000-00006
Moed BR, Willson Carr SE, Watson JT. Results of operative treatment of fractures of the posterior wall of the acetabulum. J Bone Joint Surg Am 2002;84:752-58. DOI: https://doi.org/10.2106/00004623-200205000-00008
Negrin LL, Seligson D. Results of 167 consecutive cases of acetabular fractures treated in a level one trauma center: factors associated with outcome. J Orthop Traumatol 2017;18:207-13. DOI: https://doi.org/10.1186/s13018-017-0563-6
Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. DOI: https://doi.org/10.1136/bmj.n71
Schaffer JM, Sathy AK, Engel EC, et al. Sciatic nerve palsy after operative treatment of acetabular fractures. J Orthop Trauma 2024;38:e1-8.
Simske NM, Engel AM, Engel LE, et al. Nerve injury with acetabular fracture fixation: incidence and factors affecting recovery. J Orthop Trauma 2019;33:e328-34. DOI: https://doi.org/10.1097/BOT.0000000000001604
Stavrakakis IM, Kritsotakis EI, Giannoudis PV, et al. Sciatic nerve injury after acetabular fractures: a meta-analysis of incidence and outcomes. Eur J Trauma Emerg Surg 2022;48:2639-54. DOI: https://doi.org/10.1007/s00068-022-01896-0
Tannast M, Najibi S, Matta JM. Two to twenty-year survivorship of the hip in 810 patients with operatively treated acetabular fractures. J Bone Joint Surg Am 2012;94:1559-67. DOI: https://doi.org/10.2106/JBJS.K.00444
Tile M. Fractures of the acetabulum. In: Schatzker J, Tile M, editors. The Rationale of Operative Fracture Care. Berlin: Springer; 2005. p. 267-318.
Wells GA, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa Hospital Research Institute. 2000.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 The Royal College of Orthopaedic Surgeons of Thailand

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.