Optimal Hematocrit Level Associated with Blood Reservation for Surgery for Hip Fracture
DOI:
https://doi.org/10.56929/jseaortho-2026-0296Keywords:
Hematocrit, Hip fracture, Blood loss, Hip surgery, Blood transfusionAbstract
Purpose: To study the optimal hematocrit level associated with blood reservation for high hip fracture surgery.
Methods: We retrospectively studied the medical records of 56 patients with hip fractures who underwent surgery at our hospital between January and December 2022. Data were collected including hematocrit levels before and after surgery at 6, 48, and 72 h. Risk factors and hematocrit levels for blood transfusion were assessed using univariate, bivariate, and multivariate analyses and receiver operating characteristic (ROC) curves to determine the associated factors and optimal hematocrit level in patients with hip fractures.
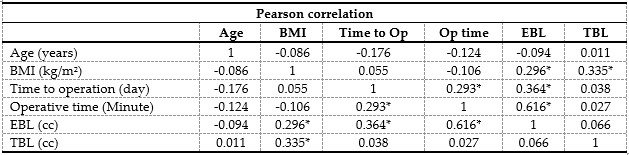
Results: Fifty-six inpatient medical records showed a statistically significant difference in age, sex, and use of antiplatelet and/or anticoagulant drugs between the blood transfusion and non- transfusion groups. The group that received antiplatelet and/or anticoagulant drugs lost significantly more blood, 191.67 ± 172.67 ml, compared with 122.86 ± 75.49 ml in those who did not receive them. In the fractures at the intertrochanter of femur, the least intraoperative blood loss was statistically significant, at 110.00 ± 60.74 ml. Comparison with fractures at the neck and subtrochanteric of femur, the blood loss was 210.74 ± 126.06 ml and 1 liter, respectively. When divided into subgroups according to femoral neck fractures, the Garden 1 group had the least intraoperative blood loss, with statistical significance at 88.00 ± 52.63 ml. There was a linear relationship between estimated blood loss and body mass index (kg/m2), time to operation (days), and operative time (minutes), with R = 0.724 and R2 = 0.524. When analyzing the ROC, the optimal hematocrit level for blood reservation for hip fracture surgery was ≤34%. The sensitivity, specificity, and accuracy were 85.7 %, 60%, and 84.2 %, respectively.
Conclusions: The optimal hematocrit level in blood reservation planning is ≤34%, with accuracy of 84.2%.
Metrics
References
Kanis JA, Oden A, McCloskey EV, et al. A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos Int 2012;23:2239-56. DOI: https://doi.org/10.1007/s00198-012-1964-3
Shoji A, Gao Z, Arai K, et al. 30-year trends of hip and vertebral fracture incidence in Japan: a systematic review and meta-analysis. J Bone Miner Metab 2022;40:327-36. DOI: https://doi.org/10.1007/s00774-021-01288-1
Brown CA, Starr AZ, Nunley JA. Analysis of past secular trends of hip fractures and predicted number in the future 2010–2050. J Orthop Trauma 2012;26:117-22. DOI: https://doi.org/10.1097/BOT.0b013e318219c61a
Michaëlsson K, Baron JA, Byberg L, et al. Declining hip fracture burden in Sweden 1998–2019 and consequences for projections through 2050. Sci Rep 2024;14:706. DOI: https://doi.org/10.1038/s41598-024-51363-6
Haddad BI, Hamdan M, Alshrouf MA, et al. Preoperative hemoglobin levels and mortality outcomes after hip fracture patients. BMC Surg 2023;23:266. DOI: https://doi.org/10.1186/s12893-023-02174-5
Meyer AC, Ek S, Drefahl S, et al. Trends in hip fracture incidence, recurrence, and survival by education and comorbidity: a Swedish register-based study. Epidemiology 2021;32:425-33. DOI: https://doi.org/10.1097/EDE.0000000000001321
Hamel MB, Henderson WG, Khuri SF, et al. Surgical outcomes for patients aged 80 and older: morbidity and mortality from major noncardiac surgery. J Am Geriatr Soc 2005;53:424-9. DOI: https://doi.org/10.1111/j.1532-5415.2005.53159.x
Finlayson E, Birkmeyer JD. Operative mortality with elective surgery in older adults. Eff Clin Pract 2001;4:172-7.
Fowler A, Abbott TEF, Prowle J, et al. Age of patients undergoing surgery. Br J Surg 2019;106:1012-8. DOI: https://doi.org/10.1002/bjs.11148
Centre TRCNB. Thailand Blood Service Action Plan 2022–2027: Thai Red Cross; 2022. 11 p.
Hematology TTSo. Blood Donation in the COVID-19 Era. n.d. Available from: https://tsh.or.th/Knowledge/Details/70.
Ramadanov N, Jóźwiak K, Hauptmann M, et al. Cannulated screws versus dynamic hip screw versus hemiarthroplasty versus total hip arthroplasty in patients with displaced and non-displaced femoral neck fractures: a systematic review and frequentist netw ork meta-analysis of 5703 patients. J Orthop Surg Res 2023;18:625. DOI: https://doi.org/10.1186/s13018-023-04114-8
Carson JL, Terrin ML, Noveck H, et al. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med 2011;365:2453-62. DOI: https://doi.org/10.1056/NEJMoa1012452
Tian S, Li H, Liu M, et al. Dynamic analysis of perioperative hidden blood loss in intertrochanteric fractures. Clin Appl Thromb Hemost 2019;25:1076029618823279. DOI: https://doi.org/10.1177/1076029618823279
Nadler SB, Hidalgo JH, Bloch T. Prediction of blood volume in normal human adults. Surgery 1962;51:224-32.
Gross JB. Estimating allowable blood loss: corrected for dilution. Anesthesiology 1983;58:277-80. DOI: https://doi.org/10.1097/00000542-198303000-00016
Cui H, Chen K, Lv S, et al. An analysis of perioperative hidden blood loss in femoral intertrochanteric fractures: bone density is an important influencing factor. BMC Musculoskelet Disord 2021;22:6. DOI: https://doi.org/10.1186/s12891-020-03922-x
Yu W, Zhang X, Wu R, et al. The visible and hidden blood loss of Asia proximal femoral nail anti-rotation and dynamic hip screw in the treatment of intertrochanteric fractures of elderly high-risk patients: a retrospective comparative study with a minimum 3 years of follow-up. BMC Musculoskelet Disord 2016;17:269. DOI: https://doi.org/10.1186/s12891-016-1143-3
Yu X, Zhang H, Zhang X, et al. Effects of the ratios of marrow cavity diameter to intramedullary nail diameter from different layers on blood loss during perioperative period for femoral intertrochanteric fractures. Medicine (Baltimore) 2019;98:e16936. DOI: https://doi.org/10.1097/MD.0000000000016936
Wang T, Guo J, Hou Z. Risk factors for perioperative hidden blood loss after intertrochanteric fracture surgery in Chinese patients: a meta-analysis. Geriatr Orthop Surg Rehabil 2022;13:21514593221083816. DOI: https://doi.org/10.1177/21514593221083816
Guo J, Zhang Y, Hou Z. Intramedullary fixation does not cause a large amount of hidden blood loss in elderly patients with intertrochanteric fractures. Clin Interv Aging 2021;16:475-86. DOI: https://doi.org/10.2147/CIA.S301737
Pincus D, Ravi B, Wasserstein D, et al. Association between wait time and 30-day mortality in adults undergoing hip fracture surgery. JAMA 2017;318:1994-2003. DOI: https://doi.org/10.1001/jama.2017.17606
Rader JC. Timing of surgery in elderly hip fracture patients. Vilniaus universitetas.; 2024.
Su S, Zhang Y, Wang R, et al. Early surgery within 48 h was associated with reduced perioperative blood loss and red blood cell transfusion requirements in older patients with hip fracture: a retrospective study. Eur Geriatr Med 2023;14:1241-8. DOI: https://doi.org/10.1007/s41999-023-00834-6
Schneider M, Schäfer N, Potthoff AL, et al. Perioperative red blood cell transfusion is associated with poor functional outcome and overall survival in patients with newly diagnosed glioblastoma. Neurosurg Rev 2022;45:1327-33. DOI: https://doi.org/10.1007/s10143-021-01633-y
Ness PM, Rosche ME, Barrasso C, et al. The efficacy of type and screen to reduce unnecessary cross matches for obstetric patients. Am J Obstet Gynecol 1981;140:661-4. DOI: https://doi.org/10.1016/0002-9378(81)90200-3
Arthi R, Soundharya V, Suresh Kumar I, et al. Impact of type and screen method on turnaround time and man-hour utilization compared to conventional Coomb’s crossmatch: A cross-sectional analytical study. Cureus 2024;16:e69564. DOI: https://doi.org/10.7759/cureus.69564
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 The Royal College of Orthopaedic Surgeons of Thailand

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.